Building a resilient, holistic pharmaceutical care system using Unit dose system dispensing (UDDS) in Uganda
Authors: Josephine M. Oyella, Clinical Pharmacist; Jacinta Otine, Pharmacist; Bosco Obalim, Jacob Odora Pharmacist, St. Mary’s Hospital Lacor
Abstract
Medication omission and administrations for admitted patients had been on the rise each year using the bulk order distribution to the wards. Little was known about the cost effectiveness of using Unit dose distribution system (UDDS) intervention.
Objective: to evaluate the cost-effectiveness of unit dose distribution system to wards.
Method:
An economic evaluation was conducted retrospectively to find the cost of medicines for the past three months alongside with a prospective initiation of UDDS in the surgical ward. A daily consumption of drugs daily dispensed was recorded for three months from June- August.
Introduction
Drug administration practices at the hospital have been targeted as an area of quality improvement. A recent pilot audit was performed (2013), with reports of up to 30% of admitted patients in the wards not receiving medications as prescribed (i.e. missed doses) with a lot of wasted prepared IV medication. The unit dose system is defined as a pharmacy coordinated method of dispensing and controlling medications in health care institutions. This system is characterized by medications contained in unit dose packages, dispensed in ready-to-administer form, and not more than 24-hour supply.
Objective
The aim is to evaluate the consumption, cost, omission and types of drug prescription and administration errors in surgical and medicine ward, comparing two dispensing schemes.
Methods before UDDS
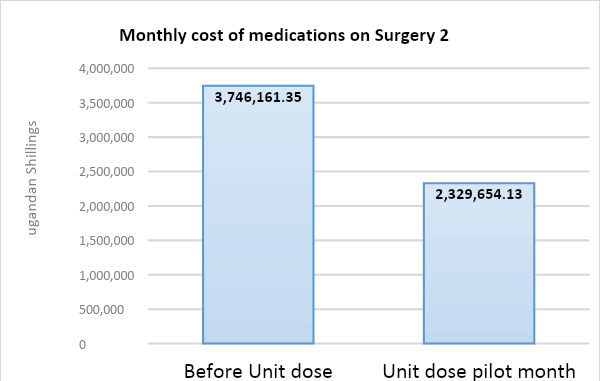
Retrospective analysis was done before UDDS from Jan-April 2019 to ascertain the average monthly consumption of drugs and its cost’ in comparison with UDDS.
Admission in June n=148, July n=142 and August n=86
Methods and Materials used during UDDS
- Criteria for unit dose daily system (UDDS)
- Pharmacist check the validity of prescription
- Medications are dispensed in units.
The medications are individually labeled and placed in separate compartment within patient drawer within the medication trolley ready for dispense. The medications are individually labeled and placed in a separate compartment within the patient drawer within the medication trolley ready for dispensed dose for administration. Medications are supplied on a daily basis, not more than 36 hours supply.
The medications are individually labeled and placed in separate compartments within the patient drawer tallying with the bed number within the medication trolley ready for dispense. (Fig 2) Another pharmacist checks the trolley to avoid omissions and errors. The medications are individually labeled and placed in separate compartment within patient drawer within the medication trolley ready for dispense.
-

- Fig. 2: Current unit dose system
-

- Fig. 2: Current unit dose system
Results
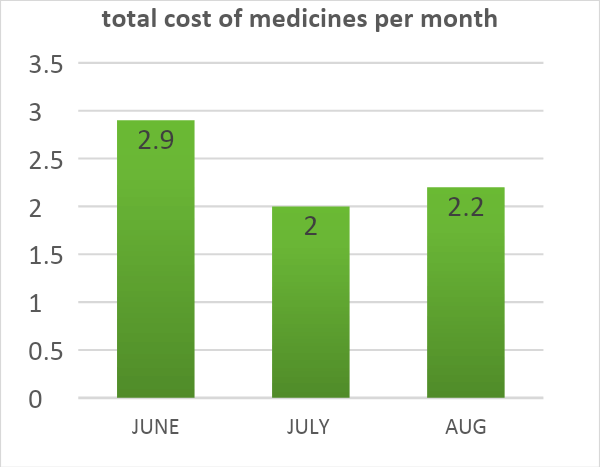
In June consumption of medicine was 4415 and decreased in July 21% as well as in August by 20%. see Table 1 illustrating the cost reduction over the three months respectively.
This is achieved due to the following: wastage of prepared IV was done at real time and given immediately, nurses waste no time in searching for medicine in the bulk cupboard, medications are packed according to prescription and put in the tray of each patient. Double checking is done by another pharmacist to avoid omission errors or wrong drug use. The UDDS system also means that medication storage is more efficient and reliable UDDS are that the pharmacy personnel are responsible for: (1) Record keeping associated with dispensing and controlling medications, (2) Interpreting physicians’ orders, (3) Maintaining patient medication records, (4) Providing unit dose packages of medications at the time the medications are to be administered. (5) In certain instances administering medications to patients.
Table 1. consumption of IV medications per month
| Medication | Consumption in June | July | August |
| IV Ampicillin | 745 | 567 | 625 |
| IV Benzyl Penicilln | 1995 | 567 | 571 |
| IV Cloxacillin | 855 | 636 | 1095 |
| IV Gentamycin | 161 | 98 | 63 |
| IV Metronidazole | 659 | 558 | 392 |
| Total | 4415 | 2426 | 2746 |
Discussions
The cost effective result in the implementation of UDDS is solely the consumption of medicines, however, there is need to demonstrate the value of hiring a pharmacist or technicians as well as equipment cost. These findings are in line with results of previous studies examining the cost-effectiveness of the combined intervention.
Drug administration is a high-risk practice in and of itself. Aside from that, medical personnel in health care facilities are under extreme time constraints. Regardless, the only thing that matters, in the end, is that the appropriate drug at the proper dosage reaches the right patient at the right time. One major advantage of unit doses is that blister packed drugs are not retrieved from the original package until it reaches the patient. This also means that no cross-contamination with other medication and human touches take place.
Conclusion
The results of the study showed that the Unit dose distribution system to the ward was substantially better suited to the needs of patient care than Ward bulk stock distribution system. The UDDS minimizes medication errors, pharmacists take full control of checking the prescriptions, improves patient safety and limit loss and pilferage and tremendously reduces cost.
References
- Bruce, Kingsley Daniel. 1976. “An Analysis of the Unit Dose Pharmacy system.” Thesis 90.
- Ding, Quian. 2012. The effect of the Unit Dose dispensing System on medication preparation. thesis, Alabama: Alabama.
- Katja Taxi, Bryony Dean & Nick Barber, 1999. “Hospital Drug Distribution Systems in the UK & Germany.” Pharmacy world & Science 25-31.