Kenya Conference of Catholic Bishops – Kenya AIDS Response Program: Management of HIV/AIDS among children
By Kennedy Indangasi, health supply chain coordinator, Kenya Conference of Catholic Bishops – Kenya AIDS Response Program (KCCB-KARP)
Management of HIV/AIDS among children by Kenya Conference of Catholic Bishops – Kenya AIDS Response Program (KCCB-KARP) By Kennedy Indangasi, Health supply chain coordinator, Kenya Conference of Catholic Bishops – Kenya AIDS Response Program (KCCB-KARP) HIV management has so far come a long way in improving the health of people living with HIV.
The government & many other organizations have partnered in providing resources to enable the fight against HIV. By this, we have seen reduced HIV infections, reduced Mother to Child Transmissions & to a great level reduced mortality for people living with HIV. Despite the many achievements, special groups still face challenges that have a far-reaching negative effect to treatment goals. These special groups include the unborn children & the young children. Treatment to this groups largely depends on maternal characters in response to health and a few health system factors.
Access to ARV medicine by Antenatal Care (ANC) mothers Prevention of mother to child transmission (PMTCT) has a lot to do with a mother having access to HIV medicine with good adherence. As much as this is a desire for the healthcare providers, we still have some mothers who due to stigma would not be willing to take medicines, some usually develop a habit of moving from one facility to another whereas posing as new clients. This in itself
compromises the quality of care to these mothers hence increasing the possibilities of having a HIV+ child since at the time of birth, they are likely to still be having high viral loads. The other challenge is seen in young girls who get pregnant at early ages & some when still in school. With the fear of disclosure for pregnancy status, these mothers shy away from getting ANC services. In the event that one was positive, chances of the client being started on treatment early enough is usually compromised.
Mitigations to the above challenges include having an empowered community health volunteers who would do house to house follow ups to link any expectant woman to care earliest possible. Preventing unwanted pregnancies goes a long way in preventing mother to child transmissions. KCCB-KARP has put in all these measures including having friendly ANC clinics to encourage mothers to get desired services timely. Support groups for ANC mother too help reduce on stigma especially for new positive clients. Traditional Birth Attendants also play a crucial role & hence their participation in HIV mentorship programs adds to the fight against mother to child transmission.
Access to ARVs by HIV positive infants
Young children treatment outcomes are vested in the ability of the mother or care giver to be committed to seeking medication for the child. Many children fail treatment entirely because they didn’t get the right treatment when they needed most. To mothers who give birth when still having the stigma to the disease, it’s likely that she won’t be free in taking the child to hospital for treatment. For the orphans & children left under the care of a different guardians, they are mostly denied access to medicine since spending time for treatment might not be a priority for them. Some might not really understand the special needs these children have especially when their work schedule goes to odd hours, it’s likely that these children will miss taking their medicines. Changing of guardians from one to another without clinic involvement again poses a challenge since not all will have the same understanding on what the child needs.
We have seen some good measure put in place to turn around these challenges. All HIV infected children are linked to their parents through PAMA (Papa Mama Care) & given special clinic days where both mother & child are seen. They have formed support groups through which they are trained on how to take care of their health & that of the child. In addition, through the support groups, they are mentored on income generating projects for sustainability. The clinic usually encourages mothers or guardians to be available at the clinic day so that they are well trained on drug dosing & storage requirement, where possible home visits are done for reinforcements.
Access to ARVs by adolescents
Most of these are school going children & some are in boarding schools. For boarding schools or some school programs make it hard for the children to access treatment at the right time. Students who keep drugs in their boxes find it hard to take medicine in the presence of others. They would wait until its dark, or when there is no one in the room for them to take their medicines. Majorly this has contributed to adherence gaps since they do not have the freedom of taking medicine. Others have their drugs kept by a certain teacher or school nurse. In the event that that teacher is not around, the child is exposed to unnecessary disclosure or still might end up delaying to take the drug at the right time or worse off ends up missing.
 Patient education on proper use of Kaletra pellets
Patient education on proper use of Kaletra pellets
We have a trend among a few adolescents who would deliberately refuse to take the medicine as a form of punishing their parents for the wrongs they did. This are the most dangerous scenarios since unless you are keen enough to understand this group, they will never open up. Clinics have organized for special youth friendly days for them to meet the sensitive demands of the group.
The boys & girls have formed OTZ (Operation Triple Zero) groups through which they are taught on adherence & health positive living. For school children, the clinics have tried follow-up in schools with mentoring of the designated teacher or nurse/matron on the care package for the child. In addition, some facilities have school-based programs where the teachers are mentored how to take care of such groups.
Supply chain challenges
Supply chain system as a whole has had some challenges that has seen facilities go without basic medicine for children or for prophylaxis. It becomes a challenge stressing to the mothers the need for proper adherence when the very medicines aren’t available. Even after availing them, the adherence message is already diluted for the period the client missed a specific drug. At times gaps in supply chain kill patients trust in a facilities health care system & promotes unnecessary transfers which even further compromises on adherence. At times treatment choices have had to be made to switch clients to available molecules which further compromises on the future options.
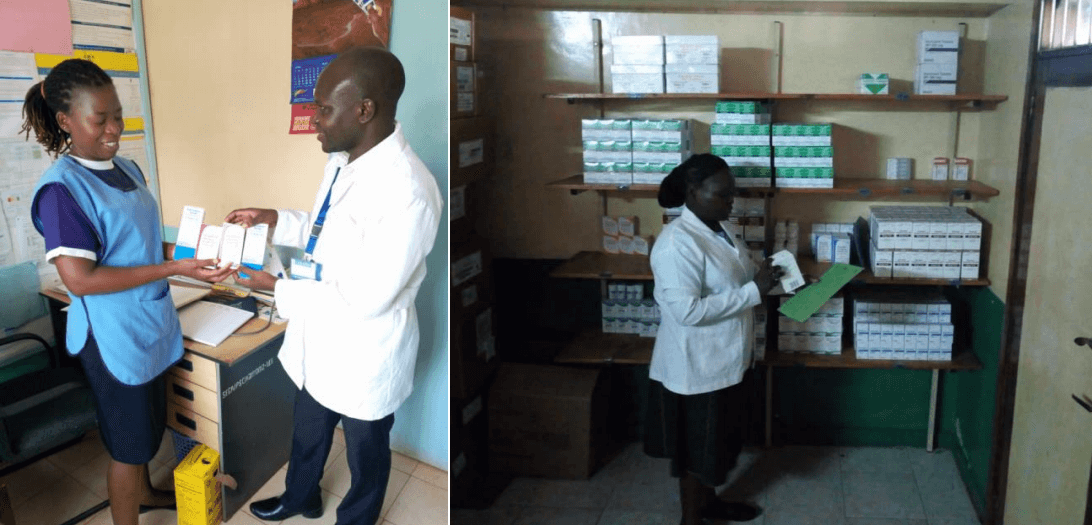
Left; Supply chain staff checking on stock status for PMTCT program at Sega Mission Hospital. Right, staff at
St. Monica clinic checks for health commodities for Children
Strengthening inventory management through supply chain mentorship programs has proven to be ideal on ensuring stock safety for all clients at all times. In addition, county collaboration through supply chain Technical Working Groups has provided an alternative to local redistributions to needy sides reducing many cases of stock outs.
Pharmaceutical Health Management systems has gone a great mile in simplifying facility inventory management processes with accurate & timely reporting that has improved the national commodity allocations. KCCB- KARP is focused on ensuring mother to child transmission is eliminated & all HIV positive children have access to the right quality care services without interruptions. Supply chain is working all round to ensure all the required medicines are available in the right proportions to avoid stock outs & overstocks.